People who snore loudly are often the target of bad jokes and middle of the night elbow thrusts; but snoring is no laughing matter. While loud disruptive snoring is at best a social problem that may strain relationships, for many men, women and even children, loud habitual snoring may signal a potentially life threatening disorder: obstructive sleep apnea, or OSA.
Snoring is not necessarily sleep apnea…
It is important to distinguish between snoring and OSA. Many people snore. It’s estimated that approximately 30% to 50% of the US population snore at one time or another, some significantly. Everyone has heard stories of men and women whose snoring can be heard rooms away from where they are sleeping.
Snoring of this magnitude can cause several problems, including marital discord, sleep disturbances and waking episodes sometimes caused by one’s own snoring. But, snoring does not always equal OSA; sometimes it is only a social inconvenience. Still, even a social inconvenience can require treatment, and there are several options available to chronic snorers.
Some non-medical treatments that may alleviate snoring include:
Weight loss — as little as 10 pounds may be enough to make a difference.
Change of sleeping position — Because you tend to snore more when sleeping on your back, sleeping on your side may be helpful.
Avoid alcohol, caffeine and heavy meals — especially within two hours of bedtime.
Avoid sedatives — which can relax your throat muscles and increase the tendency for airway obstruction related to snoring.
Your doctor has other treatment options, including the following:
Radio Frequency (RF) of the Soft Palate uses radio waves to shrink the tissue in the throat or tongue, thereby increasing the space in the throat and making airway obstruction less likely. Over the course of several treatments the inner tissue shrinks while the outer tissue remains unharmed. Several treatments may be required, but the long-term success of this procedure has not as yet been determined.
Laser-Assisted Uvuloplasty (LAUP) is a surgical procedure that removes the uvula and surrounding tissue to open the airway behind the palate. This procedure is generally used to relieve snoring and can be performed in the Oral and Maxillofacial Surgeon’s office with local or general anesthesia.
Identifying and Treating OSA
Unlike simple snoring, obstructive sleep apnea is a potentially life-threatening condition that requires medical attention. The risks of undiagnosed OSA include heart attack, stroke, irregular heartbeat, high blood pressure, heart disease and decreased libido. In addition, OSA causes daytime drowsiness that can result in accidents, lost productivity and interpersonal relationship problems. The symptoms may be mild, moderate or severe.
Sleep apnea is fairly common. One in five adults has at least mild sleep apnea and one in 15 adults has at least moderate sleep apnea. OSA also affects 1% to 3% of children. During sleep, the upper airway can be obstructed by excess tissue, large tonsils and/or a large tongue. Also contributing to the problem may be the airway muscles, which relax and collapse during sleep, nasal passages, and the position of the jaw.
The cessation of breathing, or “apnea,” brought about by these factors initiates impulses from the brain to awaken the person just enough to restart the breathing process.This cycle repeats itself many times during the night and may result in sleep deprivation and a number of health-related problems. Sleep apnea is generally defined as the presence of more than 30 apneas during a seven hour sleep. In severe cases, periods of not breathing may last for as long as 60 to 90 seconds and may recur up to 500 times a night.
Symptoms of Sleep Apnea
Those who have OSA are often unaware of their condition and think they sleep well. The symptoms that usually cause these individuals to seek help are daytime drowsiness or complaints of snoring and breathing cessations observed by a bed partner. Other symptoms may include:
Snoring with pauses in breathing (apnea)
Excessive daytime drowsiness
Gasping or choking during sleep
Restless sleep
Problem with mental function
Poor judgment/can’t focus
Memory loss
Quick to anger
High blood pressure
Nighttime chest pain
Depression
Problem with excess weight
Large neck (>17″ around in men, >16″ around in women)
Airway crowding
Morning headaches
Reduced libido
Frequent trips to the bathroom at night
Diagnosing Sleep Disorders
If you exhibit several OSA symptoms, it’s important you visit your Oral and Maxillofacial Surgeon for a complete examination and an accurate diagnosis.
At your first visit, your doctor will take a medical history and perform a head and neck examination looking for problems that might contribute to sleep-related breathing problems. An interview with your bed partner or other household members about your sleeping and waking behavior may be in order. If the doctor suspects a sleep disorder, you will be referred to a sleep clinic, which will monitor your nighttime sleep patterns through a special test called polysomnography.
Polysomnography will require you to sleep at the clinic overnight while a video camera monitors your sleep pattern and gathers data about the number and length of each breathing cessation or other problems that disturb your sleep. Often a “split night” study is done during which a C-PAP (continuous positive airway pressure) device is used. During polysomnography, every effort is made to limit disturbances to your sleep.
Treating Sleep Apnea
Obstructive sleep apnea can be effectively treated. Depending on whether your OSA is mild, moderate or severe, your doctor will select the treatment that is best for you.
Behavior Modification – If you are diagnosed with mild sleep apnea, your doctor may suggest you employ the non-medical treatments recommended to reduce snoring: weight loss; avoiding alcohol, caffeine and heavy meals within two hours of bedtime; no sedatives; and a change of sleeping positions. In mild cases, these practical interventions may improve or even cure snoring and sleep apnea.
Oral Appliances – If you have mild to moderate sleep apnea, or are unable to use C-PAP, recent studies have shown that an oral appliance can be an effective first-line therapy. The oral appliance is a molded device that is placed in the mouth at night to hold the lower jaw and bring the tongue forward. By bringing the jaw forward, the appliance elevates the soft palate or retains the tongue to keep it from falling back in the airway and blocking breathing. Although not as effective as the continuous positive airway pressure (C-PAP) systems, oral appliances are indicated for use in patients with mild to moderate OSA who prefer oral appliances, who do not respond to C-PAP, are not appropriate candidates for C-PAP, or who fail treatment attempts with C-PAP or behavioral changes.
Patients using an oral appliance should have regular follow-up office visits with their Oral and Maxillofacial Surgeon to monitor compliance, to ensure the appliance is functioning correctly and to make sure their symptoms are not worsening.
C-PAP (Continuous Positive Airway Pressure) and Bi-PAP (Bi-Level) – A C-PAP device is an effective treatment for patients with moderate OSA and the first-line treatment for those diagnosed with severe sleep apnea.Through a specially fitted mask that fits over the patient’s nose, the C-PAP’s constant, prescribed flow of pressured air prevents the airway or throat from collapsing. In some cases a Bi-PAP device, which blows air at two different pressures, may be used.
While C-PAP and Bi-PAP devices keep the throat open and prevent snoring and interruptions in breathing, they only treat your condition and do not cure it. If you stop using the C-PAP or Bi-PAP, your symptoms will return. Although C-PAP and Bi-PAP are often the first treatments of choice, they may be difficult for some patients to accept and use. If you find you are unable to use these devices, do not discontinue their use without talking to your doctor.Your Oral and Maxillofacial Surgeon can suggest other effective treatments.
Surgery for Sleep Apnea
Surgical intervention may be a viable alternative for some OSA patients; however, it is important to keep in mind that no surgical procedure is universally successful. Every patient has a different shaped nose and throat, so before surgery is considered your Oral and Maxillofacial Surgeon will measure the airway at several points and check for any abnormal flow of air from the nose to lungs. Be assured, your doctor has considerable experience and the necessary training and skill to perform the following surgical procedures:
Uvulopalatopharyngoplasty (UPPP) – If the airway collapses at the soft palate, a UPPP may be helpful. UPPP is usually performed on patients who are unable to tolerate the C-PAP. The UPPP procedure shortens and stiffens the soft palate by partially removing the uvula and reducing the edge of the soft palate.
Hyoid Suspension – If collapse occurs at the tongue base, a hyoid suspension may be indicated. The hyoid bone is a U-shaped bone in the neck located above the level of the thyroid cartilage (Adam’s apple) that has attachments to the muscles of the tongue as well as other muscles and soft tissues around the throat.The procedure secures the hyoid bone to the thyroid cartilage and helps to stabilize this region of the airway.
Genioglossus Advancement (GGA) – GGA was developed specifically to treat obstructive sleep apnea, and is designed to open the upper breathing passage. The procedure tightens the front tongue tendon; thereby, reducing the degree of tongue displacement into the throat. This operation is often performed in tandem with at least one other procedure such as the UPPP or hyoid suspension.
Maxillomandibular Advancement (MMA) – MMA is a procedure that surgically moves the upper and lower jaws forward. As the bones are surgically advanced, the soft tissues of the tongue and palate are also moved forward, again opening the upper airway. For some individuals, the MMA is the only technique that can create the necessary air passageway to resolve their OSA condition.
Talk With Your Doctor
Sleep apnea is a serious condition and individuals with OSA may not be aware they have a problem. If someone close to you has spoken of your loud snoring and has noticed that you often wake up abruptly, gasping for air, you should consult your Oral and Maxillofacial Surgeon.
The information provided here is not intended as a substitute for professional medical advice, diagnosis, or treatment. It is provided to help you communicate effectively with your oral and maxillofacial surgeon. Always seek the advice of your oral and maxillofacial surgeon regarding an oral health concern.
The American Association of Oral and Maxillofacial Surgeons (AAOMS), the professional organization representing more than 9,000 oral and maxillofacial surgeons in the United States, supports its members’ ability to practice their specialty through education, research and advocacy. AAOMS members comply with rigorous continuing education requirements and submit to periodic office examinations, ensuring the public that all office procedures and personnel meet stringent national standards.
Corrective Jaw surgery is performed by an Oral Surgeon to correct misalignment of jaw and teeth that cannot be treated with conventional Orthodontics. It is also referred to as Surgical Orthodintics. Corrective Jaw surgery improves chewing, swallowing, speech, breathing and facial apperance.
Who are Candidates for Orthognathic Surgery?
People who can benefit from orthognathic surgery include those with an improper bite or jaws that are positioned incorrectly. Jaw growth is a slow and gradual process and in some instances, the upper and lower jaws may grow at different rates causing a wide range of jaw and facial irregularities that could lead to any of these problems:
difficulty swallowing
difficulty chewing, or biting food
chronic jaw or jaw joint (TMJ) pain and headache
excessive wear of teeth
open bite (space between the upper and lower teeth when the mouth is closed)
unbalanced facial appearance from the front, or side
receding chin
inability to make the lips meet without straining
chronic mouth breathing and dry mouth
sleep apnea (breathing problems when sleeping, including snoring)
Any of these symptoms can exist at birth, be acquired after birth as a result of trauma to the face. Orthodontics alone can correct bite problems when only the teeth are involved. Orthognathic surgery may be required for the jaws when repositioning in necessary. Before any treatment begins, a consultation will be held to perform a complete examination with x-rays. During the pre-treatment consultation process, feel free to ask any questions that you have regarding your treatment. When you are fully informed about the aspects of your care, you and your dental team can make the decision to proceed with treatment together.
An oral and maxillofacial surgeon is well-trained in the treatment of facial injuries. Dr. Hutto is well versed in emergency care, acute treatment and long term reconstruction and rehabilitation. Oral and Maxillofacial Surgeons are trained, skilled and uniquely qualified to manage and treat Facial Trauma. Injuries to the face, by their very nature, impart a high degree of emotional, as well as physical trauma to patients. The science and art of treating these injuries requires special training involving a “hands on” experience and an understanding of how the treatment provided will influence the patient’s long term function and appearance. They are on staff at local hospitals and deliver emergency room coverage for facial injuries, which include the following conditions:
Facial lacerations
Intra oral lacerations
Avulsed (knocked out) teeth
Fractured facial bones (cheek, nose or eye socket)
Fractured jaws (upper and lower jaw)
The Nature of Maxillofacial Trauma
There are a number of possible causes of facial trauma such as motor vehicle accidents, accidental falls, sports injuries, interpersonal violence and work related injuries. Types of facial injuries can range from injuries of teeth to extremely severe injuries of the skin and bones of the face. Typically, facial injuries are classified as soft tissue injuries (skin and gums), bone injuries (fractures), or injuries to special regions (such as the eyes, facial nerves or the salivary glands).
Soft Tissue Injuries of the Maxillofacial Region
When soft tissue injuries such as lacerations occur on the face, they are repaired by suturing. In addition to the obvious concern of providing a repair that yields the best cosmetic result possible, care is taken to inspect for and treat injuries to structures such as facial nerves, salivary glands and salivary ducts (or outflow channels). Dr. Hutto is a well-trained oral and maxillofacial surgeon and proficient at diagnosing and treating all types of facial lacerations.
Bone Injuries of the Maxillofacial Region
Fractures of facial bones are treated in a manner similar to the fractures in other parts of the body. The specific form of treatment is determined by various factors, which include the location of the fracture, the severity of the fracture, the age and general health of the patient. When an arm or a leg is fractured, a cast is often applied to stabilize the bone to allow for proper healing. Since a cast cannot be placed on the face, other means have been developed to stabilize facial fractures.
One of these options involves wiring the jaws together for certain fractures of the upper and/or lower jaw. Certain other types of fractures of the jaw are best treated and stabilized by the surgical placement of small plates and screws at the involved site. This technique of treatment can often allow for healing and obviates the necessity of having the jaws wired together. This technique is called “rigid fixation” of a fracture. The relatively recent development and use of rigid fixation has profoundly improved the recovery period for many patients, allowing them to return to normal function more quickly.
The treatment of facial fractures should be accomplished in a thorough and predictable manner. More importantly, the patient’s facial appearance should be minimally affected. An attempt at repairing facial fractures through the fewest incisions necessary is always made. At the same time, the incisions that become necessary are designed to be small and, whenever possible, are placed so that the resultant scar is hidden.
Injuries To The Teeth and Surrounding Dental Structures
Isolated injuries to teeth are quite common and may require the expertise of various dental specialists. Oral surgeons usually are involved in treating fractures in the supporting bone or in replanting teeth that have been displaced or knocked out. These types of injuries are treated by one of a number of forms of splinting (stabilizing by wiring or bonding teeth together). If a tooth is knocked out, it should be placed in salt water or milk. The sooner the tooth is re-inserted into the dental socket, the better chance it will survive. Therefore, the patient should see a dentist or oral surgeon as soon as possible.
Never attempt to wipe the tooth off, since remnants of the ligament that hold the tooth in the jaw are attached and are vital to the success of replanting the tooth. Other dental specialists may be called upon such as endodontists, who may be asked to perform root canal therapy, and/or restorative dentists who may need to repair or rebuild fractured teeth. In the event that injured teeth cannot be saved or repaired, dental implants are often now utilized as replacements for missing teeth.
The preparation of your mouth before the placement of a prosthesis is referred to as pre-prosthetic surgery. Some patients require minor oral surgical procedures before receiving a partial or complete denture, in order to ensure the maximum level of comfort. A denture sits on the bone ridge, so it is very important that the bone is the proper shape and size. If a tooth needs to be extracted, the underlying bone might be left sharp and uneven. For the best fit of a denture, the bone might need to be smoothed out or reshaped. Occasionally, excess bone needs to be removed or recontoured prior to denture insertion.
One or more of the following procedures might need to be performed in order to prepare your mouth for a denture:
bone smoothing and reshaping
removal of excess bone
bone ridge reduction
removal of excess gum tissue
grafting of skin or specialized gum tissue
We will review your particular needs with you during your appointment.
Why is my tooth impacted?
Although all adult teeth should be erupted by the early teenage years, occasionally some teeth can fail to erupt and remain in the jaw bone. This is referred to as an impacted tooth. There can be several reasons as to why the tooth did not to erupt. Dr. Hutto will review the reasons as it pertains to your situation.
What can be done to bring my tooth into my mouth?
The procedure to correct an unerupted, impacted tooth is known as exposure and bracket. Dr. Hutto will locate the impacted tooth and bond, or glue, a special orthodontic bracket to the impacted tooth. The bracket has a chain attached to it that will allow your orthodontist to bring your tooth into proper alignment in just a matter of a few months.
Is the procedure painful?
No, typically the procedure is not painful. This procedure can be performed with local anesthesia, with nitrous oxide anesthesia, or with general anesthesia. There may be minor discomfort experienced during the recovery period. Dr. Hutto will provide you with an in-depth consultation to review all aspects of the procedure.
Your general dentist or specialist may determine that one or several teeth need to be removed for any number of reasons. Some teeth are extracted due to severe decay; others may have advanced periodontal (gum) disease, or they may be fractured in a way that cannot be repaired. Additionally, teeth may require extraction because they are poorly positioned in the mouth (such as impacted teeth), or in preparation for orthodontic treatment.
Teeth removal can lead to future changes in your chewing capability and efficiency, potential problems with your jaw joint, and the likely shifting of remaining teeth, which can have a significant impact on your overall dental health.
To avoid these potential complications, Dr. Hutto will discuss alternatives to tooth removal as well as several tooth replacement options (such as partial dentures, bridges or implants).
The Extraction Process
At the time of extraction procedure, the doctor will need to numb your tooth, jawbone and gums that surround the area with a local anesthetic. You may choose to have the surgery completed under local anesthesia alone, or in combination with nitrous oxide and moderate to deep sedation anesthesia.
During the extraction process you will likely feel a lot of pressure from the process of firmly moving the tooth in order to widen the surrounding bone socket for complete removal. However, while pressure is expected, sharp pain is not. If you do feel pain at any time during the extraction, please let us know right away.
Tooth Sectioning
Some teeth require sectioning, where the tooth is separated into smaller root pieces. Previously fractured and root canal treated teeth usually require surgical exposure and sectioning. This is commonly done when a tooth is very firmly anchored in its socket, the roots may be curved and the bone socket can’t expand adequately. The doctor simply cuts the tooth into sections then removes each section one at a time. Once all of the tooth roots and pieces are removed, the bone will be smoothed out and sutures will likely be placed to permit adequate gum healing.
If an implant is going to be eventually used to replace the now extracted tooth, Dr. Hutto will discuss the possible need to place a bone graft into the immediate extraction site to ensure that enough bone will be present after approximately 3-4 months of healing to accommodate dental implant placement.
By the age of 18, most adults have 32 teeth; 16 teeth on the top and 16 teeth on the bottom. Each tooth in the mouth has a specific name and function. The teeth in the front of the mouth (incisors, canine, and bicuspid teeth) are ideal for grasping and biting food into smaller pieces. The back teeth (molar teeth) are used to grind food up into a consistency suitable for swallowing.
The average mouth is made to hold only 28 teeth. It can be painful when 32 teeth try to fit in a mouth that holds only 28 teeth. These four other teeth are your third molars, also known as “wisdom teeth.” These can become problematic.
Why Should I Have My Wisdom Teeth Removed?
Wisdom teeth are the last teeth to erupt within the mouth. When they align properly and gum tissue is healthy, wisdom teeth do not have to be removed. Unfortunately, this does not generally happen. The extraction of wisdom teeth is necessary when they are prevented from properly erupting within the mouth. They may grow sideways, partially emerge from the gum, and even remain trapped beneath the gum and bone. Impacted teeth can take many positions in the bone as they attempt to find a pathway that will allow them to successfully erupt.
These poorly positioned impacted teeth can cause many problems. When they are partially erupted, the opening around the teeth allows bacteria to grow and will eventually cause an infection. The result: swelling, stiffness, pain, and illness. The pressure from the erupting wisdom teeth may move other teeth and disrupt the orthodontic or natural alignment of teeth. The most serious problem occurs when tumors or cysts form around the impacted wisdom teeth, resulting in the destruction of the jawbone and healthy teeth. Removal of the offending impacted teeth usually resolves these problems. Early removal is recommended to avoid such future problems and to decrease the surgical risk involved with the procedure.
What is Bone Grafting?
Bone grafting is a procedure used to replace bone and promote new bone growth. Bone grafts are often performed in coordination with the placement of dental implants. During a bone graft, bone material is placed in an area of low bone mass. In most cases, this bone material is a powder, granule, putty, or gel that has been manufactured in a lab. In some cases, the bone material may also be harvested from another location on your body. Once the bone material has been placed, it will initiate a process to produce new bone in that area.
There are different types of bone grafts, including:
Minor Bone Graft
Minor bone grafts are performed after a tooth extraction and simply place bone material in the empty tooth socket to encourage bone growth in the socket as the extraction site heals.
Medium Bone Graft
Medium bone grafts are performed when bone loss has affected the height and width of the jawbone. In this case, bone material is used to build up the height and width of the jawbone. This is one of the more common types of bone grafts.
Major Bone Graft
Major bone grafts are performed in cases of severe bone loss. A major bone graft uses a piece of bone from elsewhere in the body attached with plates and screws. Bone material is then placed around the junctions between the jawbone and donor bone to promote an even junction while healing.
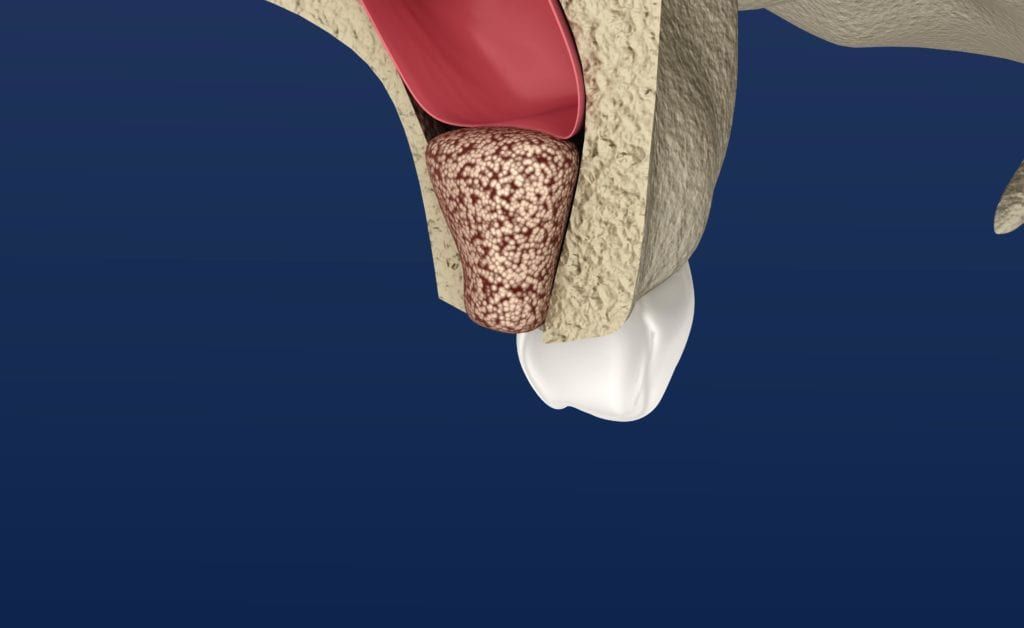
Sinus Lift
A sinus lift is a special type of bone graft that is performed on the upper jaw. With a sinus lift, bone material is added to the upper jaw in order to thicken the bone between the mouth and sinus cavity. During a sinus lift, your oral surgeon will make an incision in the gums to access the sinus cavity. Then, they will lift the sinus membrane and place bone material between the membrane and sinus floor to thicken the bone.
Why do I need a bone graft?
When one or more teeth are missing, the jawbone no longer receives stimulation from chewing. Without proper stimulation, the bone mass in that area atrophies and is reabsorbed by the body in a process known as bone resorption. Bone resorption is an irreversible process that will eventually result in structural changes to the surrounding bone structure. This also causes the quality and quantity of the remaining bone to be poor and not suitable for the placement of dental implants. In these situations, a bone graft is necessary to build up the bone structure so that dental implants can be placed.
Bone grafts are also sometimes performed to save teeth that have become loose from severe periodontitis. Unfortunately, advanced gum disease can cause the same type of bone loss associated with missing teeth. This causes the existing teeth to become loose and eventually fall out. In these cases, bone grafts can be used to regenerate the bone and secure the teeth.
In cases where teeth need to be extracted due to damage, decay, or gum disease, bone grafting material may be placed at the extraction site. This is a proactive measure that prevents bone loss and allows the patient to replace their missing tooth with a dental implant at some point in the future.
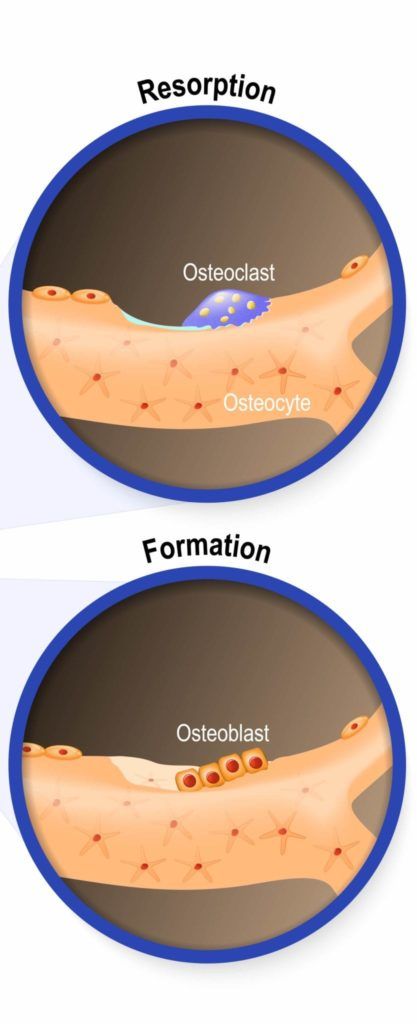
In the resorption image, you can see the presence of osteoclasts, whose main function is to help the body absorb bone material. Notice the indentation on the bone surface from a loss of bone mass. Conversely, the formation picture shows the presence of osteoblasts, whose main function is to help the body grow new bone cells. Missing teeth cause your jaw to look like the first picture, while a bone graft reverses this process and promotes new bone formation.
How is a bone graft performed?
A bone graft is a minor oral surgery that is performed with the use of dental anesthetics and sedation. In most cases, only local anesthesia is required, however deeper sedation can be used if necessary. Your oral surgeon will make a tiny incision in the gums to access the underlying bone. Then, the bone graft material will be placed in the affected area.
How long does a bone graft take to heal?
After your bone graft, the initial recovery period is about two weeks. During this period, your Modesto oral surgeon will provide you with post-operative guidelines to follow. However, bone grafts take about 3-6 months to completely heal to the point where a dental implant can be placed.
Rarely do we think about our teeth – until we lose one, or more than one, or all of them! Missing teeth can adversely affect how we chew, talk, smile and communicate. Our smile is among the very first things we focus on when we first meet other people and you can bet that many missing teeth are noticed within seconds of our opening our mouths.
Fortunately, dental implant supported restorations are changing the way people live. They are designed to replace the lost tooth roots and provide a solid foundation for replacement teeth that look, feel and function like natural teeth. The person who has lost teeth regains the ability to eat virtually anything, knowing our appearance will be preserved. Patients with dental implants can once again chew, talk and smile with confidence.
What are Dental Implants?
Dental implants are specially made titanium posts (or screws) that are surgically placed into the jawbone and are designed to integrate with the supporting bone. The implant replaces the previous tooth’s roots and provides a strong foundation for a fixed (permanent) or removable replacement tooth or teeth that should match your natural teeth.
What are the Advantages of Dental Implants?
There are many advantages to dental implants, including:
Improved appearance. Dental implants look and feel like your own teeth. And because they are designed to fuse with bone, they become permanent. In addition, implants help preserve the supporting facial bone structure. Whenever a tooth is lost, the supporting bone will resorb along with it.
Improved speech. Trying to speak clearly without your front teeth is a major challenge. Over time, with poor-fitting dentures, false teeth can slip within the mouth causing you to mumble or slur your words. Dental implants allow you to speak without the worry that teeth might slip.
Improved comfort. Because the surrounding bone fuses to the implant surface, denture wearers see immediate and profound improvement in their denture comfort, fit and function.
Easier eating. Dental implants are designed to function like natural teeth, allowing you to eat your favorite foods with confidence and comfort. Removable denture wearers are lucky to be able to obtain 25% of their previous chewing function – dental implant supported prostheses change the food choice options overnight.
Improved self-esteem. Dental implants can give you back your smile and help you feel better about yourself.
Improved oral health. Dental implants don’t require reducing other teeth, as a tooth-supported bridge does. Because nearby teeth are not altered to support the implant, more of your own teeth are left intact, improving long-term oral health. Individual implants also allow easier access between teeth, improving oral hygiene.
Durability. Implants are very durable and usually last many years. With good care, many implants last a lifetime.
Convenience. Removable dentures are just that; removable. Dental implants eliminate the embarrassing inconvenience of removing dentures, as well as the need for messy adhesives to keep them in place.
How Successful Are Dental Implants?
Success rates of dental implants vary, depending on multiple factors such as where in the jaw the implants are placed, health histories and other chewing factors; however, in general, dental implants have a success rate of up to 95-98%. With proper care, many implants can last a lifetime.
Can Anyone Get Dental Implants?
In most cases, anyone healthy enough to undergo a routine dental extraction or oral surgery procedure is a potential candidates for a dental implant placement procedure. Healthy gums and adequate bony support to hold the implant are factors for long-term success. Patients must be committed to good oral hygiene and regular dental visits. Heavy smokers, people suffering from uncontrolled chronic disorders (such as diabetes), compromised immune system states, patients taking specific bone altering medications, or patients who have had previous head and neck radiation therapy need to be evaluated on an individual basis.
The Surgical Procedure
For most patients, the dental implant placement involves one surgical procedure. The implants are placed within your jawbone and a healing cap is placed on the implant. The healing cap extends through the gum tissue and helps shape the gum tissue for the eventual final crown or prosthesis.
Bone fusing to the titanium surface of the implant (called osseointegration) takes approximately 3-6 months, depending on the location of implant placement (the upper jaw has less dense bone and takes longer to integrate). During this time, a plan for the making of a temporary tooth or removable prosthesis will be followed with limited chewing occurring on the recently placed dental implant. Once the implant healing process is complete, your general dentist will then remove the healing cap, place a permanent abutment, and take impressions to begin fabricating the final restoration. Most patients experience very little change in their daily activities throughout the entire implant process.
Additional surgical procedures may be indicated depending on the condition of the jawbone where the implant is to be placed. In these cases, Dr. Hutto utilizes advanced bone grafting to prepare the jawbone for implant placement. At your initial consultation, your doctor will determine if bone grafting is needed and discuss the procedures involved. The doctor will also take time to answer any questions you may have regarding dental implant treatment.
{kind=link}